


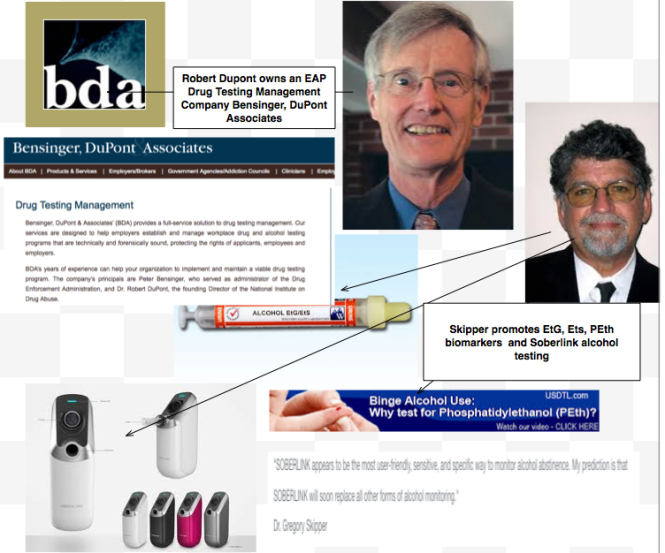
Before the 2012 Drug and Alcohol Testing Industry Association (DATIA) annual conference, former Nixon Drug Czar Dr. Robert Dupont delivered a speech entitled “Drug Testing and the Future of American Drug Policy.” Dupont describes a “New Paradigm” for substance abuse treatment that enforces “zero tolerance for alcohol and drug use” enforced by monitoring with frequent random drug and alcohol tests in which positive tests are “met with swift, certain, but not draconian, consequences.” The paradigm is based on the current Physician Health Programs blueprint. Dupont states:
“…physician health programs , have set the standard for effective use of drug testing. These pioneering state programs provide services to health care professionals with substance use disorders. The programs are run by physicians, some of whom in recovery themselves. PHPs feature relatively brief but highly focused treatment followed by active lifelong participation in the 12-step fellowships of Alcoholics Anonymous and Narcotics Anonymous. The key to the success of the PHP system of care management is the enforcement of the standard of zero tolerance for any alcohol or other drug use by intensive long-term random testing for both alcohol and drugs with swift and certain consequences for even a single use of alcohol or any other drugs of abuse. PHPs use drug panels of 20 or more drugs. The PHPs commonly use EtG and EtS tests to detect recent alcohol use. Similar comprehensive programs have been developed for commercial pilots and attorneys. These innovative programs of care management produce unprecedented long-term, outcomes.”Physician Health Programs (PHPs) use a doctor’s medical license as “leverage” in what they call “contingency management.” The doctor must comply with any and all demands made under threat of being reported to their medical board for “non-compliance.” The national organization representing PHPs, the Federation of State Physician Health Programs (FSPHP) has convinced the national organization representing state medical boards, the Federation of State Medical Boards (FSMB) that “second-guessing” PHP authority “undermines a culture of professionalism.” As with every other ware the FSPHP has pitched the FSMB they accepted this notion in blind faith and without critical analysis. If they did look a little deeper they would find the “PHPs-blueprint” more resembles a paradigm of “racketeering” then it does “rehabilitation” or “recovery” and the terms they use are euphemisms. Taking a medical license “hostage” and holding it for “ransom” while putting coins in your pocket by “extortion” doesn’t fit in with a “culture of professionalism” though. They are very good at impression management–have to give them that.
Declaring the PHP model the “gold standard” of substance abuse treatment they now want to spread the wealth to others, including kids. But instead of a medical license it will be your student loan, right to participate in school sports, teaching license, hairdressing license, commercial truck driving license, gun license, and even license to drive they will be after. If you got it and it is in any way tied to state or federal government benefits or rights they will threaten you with removing it. And as is being seen in doctors there will not be a damned thing you will be able to do about it.
This is all outlined in the 2013 American Society of Addiction Medicine White Paper on Drug Testing. If you have not read it yet you need to. If you read one thing this year make it this as it is under the radar and no one is talking about it.
A Modest Proposal
I implore you to do two things:
1. Read the ASAM White Paper on Drug Testing in its entirety. It can be found here and here.
2. If you like what you see do nothing. If this is the predominant response then it will surely come to fruition as has every other public policy recommendation the ASAM has pushed. ( See policy entrepreneurship, bent science, moral crusades).
3. If you don’t like what you see then stand up! Make your voice known. Make your voice known in every venue you can. Write and call your local and state politicians, comment in the news media, tweet, Instagram, post to FaceBook, send links to your connections on Linkedin. Do everything you can because we do not have long. The ASAM is slated to become recognized by the American Board of Medical Specialties in 2016 and that will be the beginning of the end. What is described in the ASAM White Paper will be ushered in and, as we have seen with what has happened to doctors, there will not be a thing you will be able to do about it.
The ASAM is not a medical “specialty” but a “special interest group representing the billion dollar drug and alcohol testing, assessment and treatment industry. Although they say they exist to help addicts and benefit the public their plans as outlined below suggest they do neither. Moreover, many of the architects of this future drug-testing dystopia can be found right here on this list.
In order to prevent this we need voices now! Please take the ASAM White Paper on Drug Testing Challenge. Read it, form an opinion and state, yell and shout your opinion everywhere and anywhere you can.
The 2013 American Society of Addiction Medicine White Paper on Drug Testing describes the organizational structure of the “New Paradigm” which includes utilization of the medical profession as a urine collection agency for their drug and alcohol testing. When a doctor-patient relationship exists the testing is rendered “clinical” rather than “forensic.” Thus the consequences of a positive test can be deemed “treatment” rather than punishment. This bypasses the strict chain-of-custody and Medical Review Officer requirements designed to ensure accuracy and minimize false-positives. Forensic drug testing is tightly regulated because the results a positive test can be grave and far reaching. Erroneous results are unacceptable.
And then he proposed expansion of this paradigm to other populations including workplace, healthcare, and schools.

Chain-of-Custody refers to the document or paper trail showing the collection, control, transfer, analysis and disposition of laboratory tests. It is the written documentation of a specimen from the moment of collection to the final destination to the review and reporting of the final results. The multi-part chain-of-custody form or “custody and control” form is part and parcel of this process. It contains stickers to sign and seal the specimen so that it cannot be tampered with and the form itself is signed by the appropriate parties as the test specimen travels from place to place. Information is added to the form as it travels from person to person. It has been given the status of a legal document as it has the ability to invalidate a specimen with incomplete information. Once the sample is analyzed it is reviewed by a Medical Review Officer (MRO) for final review. In the case of a positive test it is the responsibility of the MRO to ascertain an intact chain-of-custody, determine whether an alternative explanation exists for the positive test such as a prescribed medication, and then and only then report the test as a “true positive.”
The MRO looks for what are called “fatal flaws” and, should one be present, invalidates the test. A fatal flaw requires the test be rejected as it were never drawn. It invalidates it and it cannot be used.  Any and all drug testing requires strict chain-of-custody procedures. It documents not only the whereabouts of the specimen at any given time but the management and storage of the specimen. This is important because time and temperature can influence the results of certain tests. One such test is alcohol.
Any and all drug testing requires strict chain-of-custody procedures. It documents not only the whereabouts of the specimen at any given time but the management and storage of the specimen. This is important because time and temperature can influence the results of certain tests. One such test is alcohol.
Specimen integrity is critical in forensic drug testing, but so too is the integrity of the people involved.
Forensic Versus Clinical Drug Testing
According to the ASAM White Paper on Drug Testing, clinical drug-testing “employs the same sound procedures, safeguard, and systems of information management that are used for all other health-related laboratory tests, tests on which life-and-death medical decisions are commonly made.” In the box below they describe the multiple safeguards in place and requirements demanded of “forensic” drug testing but do not mention the reason these uncompromising and multiple specifications exist is to protect the donor from a false accusation of drug or alcohol use. They proceed to define “clinical drug testing” as “part of a patient examination performed for the purposes of diagnosis, treatment, and the promotion of long term recovery” noting that clinical testing “must meet the established standards of medical practice and benefit the therapeutic relationship, rather than meeting the formal legal requirements of forensic testing.” The authors then state that the “majority of drug testing done today” includes both forensic and clinical elements using individuals on parole and probation as examples.
From the ASAM White Paper on Drug Testing
The logical fallacy here is striking. It is comparing apples and oranges. After detailing the specific quality assurance safeguards designed to prevent the donor of a drug or alcohol test from being falsely accused of illicit use, the authors give a general definition and purpose of “clinical” testing then state that when testing for drugs the systems in place are up to snuff as it is already being used to make life-and-death medical decisions. The take-home message is that “forensic” testing is unnecessary hyperbole designed for legal challenges. The clinical lab systems in place are used for critically important testing so it can be used for drug-testing. After all, parolees and probationers don’t require it.
Forensic guidelines were developed in collaboration with occupational and environmental medicine specialists, clinical and forensic toxicologists, pathologists and others and the recommended requirements agreed upon by this consortium exists solely to assure validity and accuracy in the testing process. These requirements exist to protect the donor and If the “clinical” testing context fit the bill then “forensic” testing would not have evolved.
Labs ordered clinically in the course of patient care are interpreted within the context of multiple other pieces of data. Lab errors occur all the time and are interpreted in that context. Oftentimes a lab will not fit with the clinical picture and, when that happens, a repeat lab is ordered for verification. Specimens get collected in the wrong tube and specimens get lost but in the clinical setting they simply get reordered and there are no consequences to patient care. In contrast drug testing is an all-or-none one-shot test and the results have consequences. It is for that reason they must be valid. Chain-of-custody and MRO review are critical and that is why most drug-testing programs follow the forensic protocol. And the example of non-forensic drug-testing parolees and probationers is misleading. Any Employee Assistance Program that has a union or some other group looking out for their best interests uses strict “forensic” guidelines. Parolees and probationers have no power and have no choice. Besides, the National Association of Drug Court Professionals uses the Laboratory Developed Tests these same people introduced to test individuals on probation or parole in the criminal justice system just as they do in the PHPs.
The ASAM White Paper:
“Encourages wider and “smarter” use of drug testing within the practice of medicine and, beyond that, broadly within American society. Smarter drug testing means increased use of random testing* rather than the more common scheduled testing,* and it means testing not only urine but also other matrices such as blood, oral fluid (saliva), hair, nails, sweatand breath when those matrices match the intended assessment process. In addition, smarter testing means testing based upon clinical indication for a broad and rotating panel of drugs”
As a physician-patient relationship renders drug testing “clinical” rather than “forensic” the consequences become “treatment” rather than “discipline.” And that is the real reason behind all of this. A positive “forensic” test in most employee random drug screening programs today will result in an “assessment” for substance abuse. Most EAPs allow a choice in where that assessment takes place. The model this system is based on, Physician Health Programs. does not allow choice as evaluations are mandated to “PHP-approved” assessment centers; a rigged game.
A positive “clinical” test will result in the same thing under the ASAM White Paper proposal. But the assessment will be at an ASAM facility and if a Substance Use Disorder (SUD) is confirmed it will result in mandated abstinence of all substances (including alcohol) and lifelong spirituality involving 12-step recovery And by using the healthcare system as a loophole and calling this testing “clinical” rather than “forensic” the ASAM will have successfully introduced widespread testing of a variety of Laboratory Developed Tests (LDTs) of unknown validity while removing the safeguards provided by forensic testing including chain-of-custody and MRO review.



This is confusing and an invasion of rights. Not only that but it seems as if the Pharmaceuticals will get rich off of testing supplies and the redos of tests to confirm a dx.
LikeLike
That’s the plan. And this is what we are up against. A lot of people will be getting rich on this.
http://www.abamfoundation.org/our_initatives/
LikeLiked by 1 person
Reblogged this on U.S. Marijuana Party.
LikeLiked by 1 person
Thanks for re-blogging. I reviewed all of ASAM regarding MMJ public policy. The plan is for the ASAM and the FSPHP to recommend both public policy and changes to state Administrative Practice and Medical Practice Acts that mandate any doctor who counsels an MMJ patient be an “addiction medicine” specialist under the (false) premise of authority in that these doctors have the “special knowledge and experience” to do so.
The ASAM/FSPHP and state physician health programs play a powerful yet unseen role in MMJ regulation. Although hidden they pull the strings at the medical boards, medical societies and departments of public health. They also have a strong alliance with the DEA.
The underlying current of fear also pervades medicine. Many MMJ activists are blaming “doctors” for not speaking up. Take a look at the article below concerning NJ.
http://www.nj.com/politics/index.ssf/2014/06/medical_marijuana_programs_slow_enrollment_worries.html
Doctors are afraid to have their name on a website out of fear of being pulled in by the Medical Society PHP. This has already happened to a friend of mine in Oregon. All it takes is an anonymous complaint to bring you in and that is what they did to him.
I also know of two doctors who were involved in MMJ who were pulled over driving, referred to their state PHP and ultimately diagnosed with a (non-existent) diagnosis of substance abuse by one of the “PHP-approved” assessment and treatment centers.
Things like this effectively silence the voices of the rest. As with all of the other chicanery and misconduct this is all hiding in plain site. The ASAM/FSPHP is not a medical specialty but a “special interest group” representing the drug and alcohol testing, assessment and treatment industry (Each billion dollar enterprises).
They represent prohibition, the drug war and are anti harm-reduction and anti -MMJ. This paradigm supports how they profit and it is static, stagnant and not amenable to reason, fact or science.
The ASAM is the public outreach and education arm of the front-group. The FSPHP is the private “muscle.” The FSPHP are the “Brown-shirts” for prohibition if you will. They are unregulated, accountable to no one, and under multiple layers of immunity, impunity, and opacity.
Click to access Gundersen%20Presentation.pdf
Click to access Dinnan%20Presentation.pdf
President Comments on Marijuana Use, ASAM Expresses Concern
CHEVY CHASE, MD, JANUARY 21, 2014 – The American Society of Addiction Medicine (ASAM) expresses its concern that the President’s comments regarding marijuana use, in the January 27, 2014 edition of The New Yorker magazine, may contribute to the growing misperception among America’s youth that marijuana is harmless.
ASAM, the largest American medical professional society dedicated to the treatment and prevention of addiction, has examined both the medical and recreational use of marijuana and the public health consequences of both. In neither case, did the Society find sufficient evidence to support the notion that the public health benefits of using the illicit drug outweighed the dangers to users and to their communities. According to the National Institute on Drug Abuse, marijuana is an intoxicating drug that impairs memory, motor function, and, when smoked, respiratory health. And, for nearly one in ten habitual users, marijuana is addictive.
“Addiction is a chronic brain disease that can affect people at any age. In fact, the younger one initiates alcohol or drug use, the greater the likelihood that he or she has addictive disease,” says Dr. Stuart Gitlow, ASAM’s President. “The addicted brain doesn’t care if the substance is alcohol or marijuana; both can be very dangerous, particularly to the naïve user.”
ASAM respects the President’s concerns regarding inequitable drug-related criminal sentencing policies and has long held a policy that treatment is a more appropriate response to minor drug-related criminal offenses than incarceration. “Public policies that support prevention and treatment for addiction should be the basis of our government’s response to a chronic disease that affects 23 million Americans,” offers Dr. Gitlow. “This requires, however, that substances of abuse are not made more easily available or made to seem less dangerous than they really are.”
ASAM encourages the President and our nation’s policy makers to build public awareness for addiction prevention and treatment, whether the addictive substance is alcohol, nicotine, marijuana or prescription opioids. ASAM looks forward to working with the Administration and state and federal policymakers to advance science-based policies that deter unhealthy substance use and promote access to treatment for those that need it.
I have not covered these issues yet but it they are on the roster. If there is any way you can take a look, fact check and help me get it out there please do. I need allies.
LikeLiked by 1 person
I will gladly repost anything you write. If you could forward to me via email at shereekrider@usmjparty.com it would be great. I have a lot of blogs and information to cover on a lot of subjects here in Kentucky….I do not always get to the information I need right away via “blog surfing”….I read too much! Anyway, the short answer is YES!
Sheree Krider
LikeLike
Thanks Sheree– See this http://50.56.238.19/boston-news-opinions/2013/05/blunt-truth-ma-dph-doctors-might-as-well-be-scientologists/
LikeLike
Candidates are getting hammered on the campaign trail with “My daughter died of opiate addiction” stories. Docs and pain patients must hammer back or we’ll be reading our worst fears off both candidates’ campaign platforms!
LikeLike
Yes, they are using the same logical fallacy by arguing that a bad outcome would not have occurred if the person had 60 days of inpatient treatment. And the evidence-base they are claiming supports what they push is very poor. The logical fallacy needs to be pointed out by credible experts and these irrational and illegitimate fake experts need to be exposed. It would not be that hard as the science is so below par it boggles the mind but everyone remains silent. Take a position. Anyone who remains “neutral” in this is complicit. Peoples lives are on the line. For God’s sake say something. Either support them or speak out against them it is as simple as that.
LikeLike
OK but they are also arguing for a crackdown on opiate prescriptions. Which is already happening and is already killing people. How? Because people in chronic pain are already on the verge of suicide and nothing like cutting them off to push them over the edge. Thank god for heroin at least.
LikeLiked by 1 person
It is unbelievable– they want opiates only for cancer and then want conservative management of that. I know of multiple elderly patients well managed on low dose opiates who are now cutoff
LikeLiked by 1 person
Reblogged this on artbylisabelle and commented:
The Medical Industrial Complex is hungry. American citizens are no longer individuals with rights, we are all Big Pharma’s patients. We are not a country of men and women, we are patients. Welcome to the United Nation States of Big Pharma, the new world order! We are under the scrutiny and microscope of a profit driven out-of-control oligarchy that will dominate every facet and second of our lives!
LikeLiked by 1 person
Reblogged this on Disrupted Physician.
LikeLike
I read through this white paper in some detail. “Sickening”, “chilling”, and “dystopian” are all adjectives that come to mind. These people represent the brain trust in the war on drugs. I am going to have calm myself a bit before raising specific objections.
There is trouble in River City to be sure. And River City is everywhere.
LikeLiked by 1 person
Yet ignorance is bliss. It’s written out in detail and they are already giving courses on the “new paradigm. “Addiction Medicine is slated to become accepted by ABMS as a true specialty in 2016. At that time the locusts will infest the system and the White Paper nightmare begins for everyone else
LikeLike
Reblogged this on Chaos Theory and Pharmacology.
LikeLiked by 1 person