


Chain-of-Custody refers to the document or paper trail showing the collection, control, transfer, analysis and disposition of laboratory tests. It is the written documentation of a specimen from the moment of collection to the final destination to the review and reporting of the final results. The multi-part chain-of-custody form or “custody and control” form is part and parcel of this process. It contains stickers to sign and seal the specimen so that it cannot be tampered with and the form itself is signed by the appropriate parties as the test specimen travels from place to place. Information is added to the form as it travels from person to person. It has been given the status of a legal document as it has the ability to invalidate a specimen with incomplete information. Once the sample is analyzed it is reviewed by a Medical Review Officer (MRO) for final review. In the case of a positive test it is the responsibility of the MRO to ascertain an intact chain-of-custody, determine whether an alternative explanation exists for the positive test such as a prescribed medication, and then and only then report the test as a “true positive.”
The MRO looks for what are called “fatal flaws” and, should one be present, invalidates the test. A fatal flaw requires the test be rejected as it were never drawn. It invalidates it and it cannot be used.  Any and all drug testing requires strict chain-of-custody procedures. It documents not only the whereabouts of the specimen at any given time but the management and storage of the specimen. This is important because time and temperature can influence the results of certain tests. One such test is alcohol.
Any and all drug testing requires strict chain-of-custody procedures. It documents not only the whereabouts of the specimen at any given time but the management and storage of the specimen. This is important because time and temperature can influence the results of certain tests. One such test is alcohol.
Specimen integrity is critical in forensic drug testing, but so too is the integrity of the people involved.
Forensic Versus Clinical Drug Testing
According to the ASAM White Paper on Drug Testing, clinical drug-testing “employs the same sound procedures, safeguard, and systems of information management that are used for all other health-related laboratory tests, tests on which life-and-death medical decisions are commonly made.” In the box below they describe the multiple safeguards in place and requirements demanded of “forensic” drug testing but do not mention the reason these uncompromising and multiple specifications exist is to protect the donor from a false accusation of drug or alcohol use. They proceed to define “clinical drug testing” as “part of a patient examination performed for the purposes of diagnosis, treatment, and the promotion of long term recovery” noting that clinical testing “must meet the established standards of medical practice and benefit the therapeutic relationship, rather than meeting the formal legal requirements of forensic testing.” The authors then state that the “majority of drug testing done today” includes both forensic and clinical elements using individuals on parole and probation as examples.
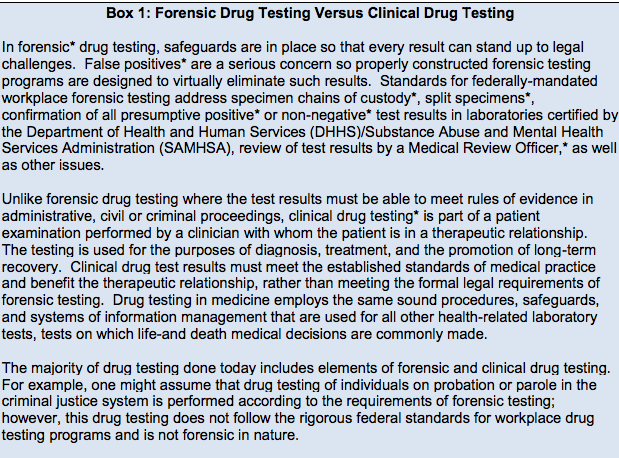
From the ASAM White Paper on Drug Testing
The logical fallacy here is striking. It is comparing apples and oranges. After detailing the specific quality assurance safeguards designed to prevent the donor of a drug or alcohol test from being falsely accused of illicit use, the authors give a general definition and purpose of “clinical” testing then state that when testing for drugs the systems in place are up to snuff as they are already being used to make “life-and-death medical decisions.” The take-home message is that “forensic” testing is unnecessary hyperbole designed for legal challenges. The clinical lab systems in place are used for critically important testing and can therefore be used for drug-testing–after all, parolees and probationers don’t require it.
Forensic guidelines were developed in collaboration with occupational and environmental medicine specialists, clinical and forensic toxicologists, pathologists and others and the recommended requirements agreed upon by this consortium exists solely to assure validity and accuracy in the testing process. These requirements exist to protect the donor and If the “clinical” testing context fit the bill then “forensic” testing would not have evolved.
Labs ordered clinically in the course of patient care are interpreted within the context of multiple other pieces of data. Lab errors occur all the time and are interpreted in that context. Oftentimes a lab will not fit with the clinical picture and, when that happens, a repeat lab is ordered for verification. Specimens get collected in the wrong tube and specimens get lost but in the clinical setting they simply get reordered and there are no consequences to patient care. In contrast drug testing is an all-or-none one-shot test and the results have consequences. It is for that reason they must be valid. Chain-of-custody and MRO review are critical and that is why most drug-testing programs follow the forensic protocol. And the example of non-forensic drug-testing parolees and probationers is misleading. Any Employee Assistance Program that has a union or some other group looking out for their best interests uses strict “forensic” guidelines. Parolees and probationers have no power and have no choice. Besides, the National Association of Drug Court Professionals uses the Laboratory Developed Tests these same people introduced to test individuals on probation or parole in the criminal justice system just as they do in the PHPs.
The ASAM White Paper:
“Encourages wider and “smarter” use of drug testing within the practice of medicine and, beyond that, broadly within American society. Smarter drug testing means increased use of random testing* rather than the more common scheduled testing,* and it means testing not only urine but also other matrices such as blood, oral fluid (saliva), hair, nails, sweatand breath when those matrices match the intended assessment process. In addition, smarter testing means testing based upon clinical indication for a broad and rotating panel of drugs”
As a physician-patient relationship renders drug testing “clinical” rather than “forensic” the consequences become “treatment” rather than “discipline.” And that is the real reason behind all of this. A positive “forensic” test in most employee random drug screening programs today will result in an “assessment” for substance abuse. Most EAPs allow a choice in where that assessment takes place. The model this system is based on, Physician Health Programs. do not allow choice as evaluations are mandated to “PHP-approved” assessment centers; a rigged game.
A positive “clinical” test will result in the same thing under the ASAM White Paper proposal. But the assessment will be at an ASAM facility and if a Substance Use Disorder (SUD) is confirmed it will result in mandated abstinence of all substances (including alcohol) and lifelong spirituality involving 12-step recovery And by using the healthcare system as a loophole and calling this testing “clinical” rather than “forensic” the ASAM will have successfully introduced widespread testing of a variety of Laboratory Developed Tests (LDTs) of unknown validity while removing the safeguards provided by forensic testing including chain-of-custody and MRO review.


Yikes. Scary stuff.
LikeLiked by 1 person
Reblogged this on theperfectprescription2014.
LikeLiked by 1 person
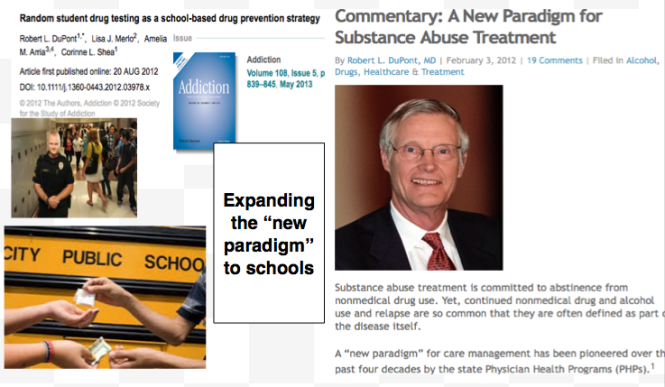
[…] tests for drug and alcohol testing into healthcare via a loophole. This same group introduced most of these tests through a loophole and now want to TEST EVERYBODY including students and kids through another […]
LikeLike
[…] Laboratory Developed Tests (LDTs) into mainstream healthcare via a loophole. This same group introduced most of these tests through a loophole and now they want to drug-and alcohol TEST EVERYBODY including STUDENTS AND KIDS through another […]
LikeLike
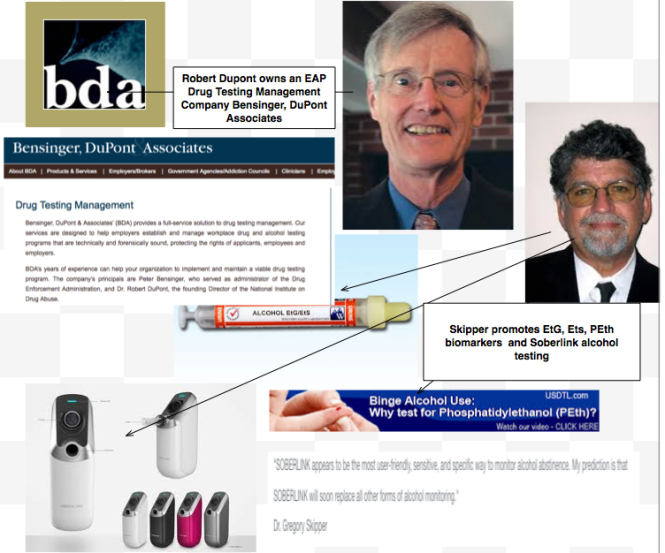
[…] State PHP programs require strict adherence to 12-step doctrine9 yet many of the physicians monitored by them are neither addicts nor alcoholics. Some do not even have substance abuse issues and there are reports of “disruptive” physicians being diagnosed with “character defects” at the “PHP-approved” facilities that do these assessments. PHPs require abstinence from drugs and alcohol yet used non-FDA approved Laboratory Developed Tests in their monitoring programs. Many of these tests were introduced to commercial labs and promoted by ASAM/FSPHP physicians.10-12 […]
LikeLike
[…] Laboratory Developed Tests (LDTs) into mainstream healthcare via a loophole. This same group introduced most of these tests through a loophole and now they want to drug-and alcohol TEST EVERYBODY including STUDENTS AND KIDS through another […]
LikeLike
Reblogged this on Citizens, not serfs.
LikeLiked by 1 person
Reblogged this on markcatlin3695's Blog.
LikeLiked by 1 person
[…] Paradoxically, laboratory developed tests with the potential to cause life-changing and possibly irreparable harm have been absent from the regulatory debate; LDT drug and alcohol tests used for “forensic” monitoring purposes. […]
LikeLiked by 1 person
[…] State PHP programs require strict adherence to 12-step doctrine9 yet many of the physicians monitored by them are neither addicts nor alcoholics. Some do not even have substance abuse issues and there are reports of “disruptive” physicians being diagnosed with “character defects” at the “PHP-approved” facilities that do these assessments. PHPs require abstinence from drugs and alcohol yet use non-FDA approved Laboratory Developed Tests in their monitoring programs. Many of these tests were introduced to commercial labs and promoted by ASAM/FSPHP physicians.10-12 […]
LikeLike
[…] State PHP programs require strict adherence to 12-step doctrine9 yet many of the physicians monitored by them are neither addicts nor alcoholics. Some do not even have substance abuse issues and there are reports of “disruptive” physicians being diagnosed with “character defects” at the “PHP-approved” facilities that do these assessments. PHPs require abstinence from drugs and alcohol yet use non-FDA approved Laboratory Developed Tests in their monitoring programs. Many of these tests were introduced to commercial labs and promoted by ASAM/FSPHP physicians.10-12 […]
LikeLike
[…] State PHP programs require strict adherence to 12-step doctrine9 yet many of the physicians monitored by them are neither addicts nor alcoholics. Some do not even have substance abuse issues and there are reports of “disruptive” physicians being diagnosed with “character defects” at the “PHP-approved” facilities that do these assessments. PHPs require abstinence from drugs and alcohol yet use non-FDA approved Laboratory Developed Tests in their monitoring programs. Many of these tests were introduced to commercial labs and promoted by ASAM/FSPHP physicians.10-12 […]
LikeLike
Reblogged this on Disrupted Physician and commented:
The logical fallacy here is striking. It is comparing apples and oranges. After detailing the specific quality assurance safeguards designed to prevent the donor of a drug or alcohol test from being falsely accused of illicit use, the authors give a general definition and purpose of “clinical” testing then state that when testing for drugs the systems in place are up to snuff as it is already being used to make life-and-death medical decisions. The take-home message is that “forensic” testing is unnecessary hyperbole designed for legal challenges. The clinical lab systems in place are used for critically important testing so it can be used for drug-testing. After all, parolees and probationers don’t require it.
LikeLike
[…] Mandating Drug-Testing of Unknown Validity while removing the procedural safeguards of forensic drug… […]
LikeLike
[…] Source: Mandating Drug-Testing of Unknown Validity while removing the procedural safeguards of forensic drug… […]
LikeLike
[…] Source: Mandating Drug-Testing of Unknown Validity while removing the procedural safeguards of forensic drug… […]
LikeLike
Hi Michael, I can’t reblog it, I am going to update my wordpress plan (maybe is because of that) or perhaps is a new configuration in your blog? please let me know, cheers!
LikeLike
Hi Jorge – it seems set correctly. Let me know
LikeLiked by 1 person
Reblogged this on Chaos Theory and Pharmacology.
LikeLike